Heart and Cardiometabolic Health
How statins, cholesterol, and diet really fit cardiovascular risk.
Get Beyond Cholesterol, free
A plain-English guide to why a basic cholesterol panel falls short, and the three ways to see your real cardiovascular risk.
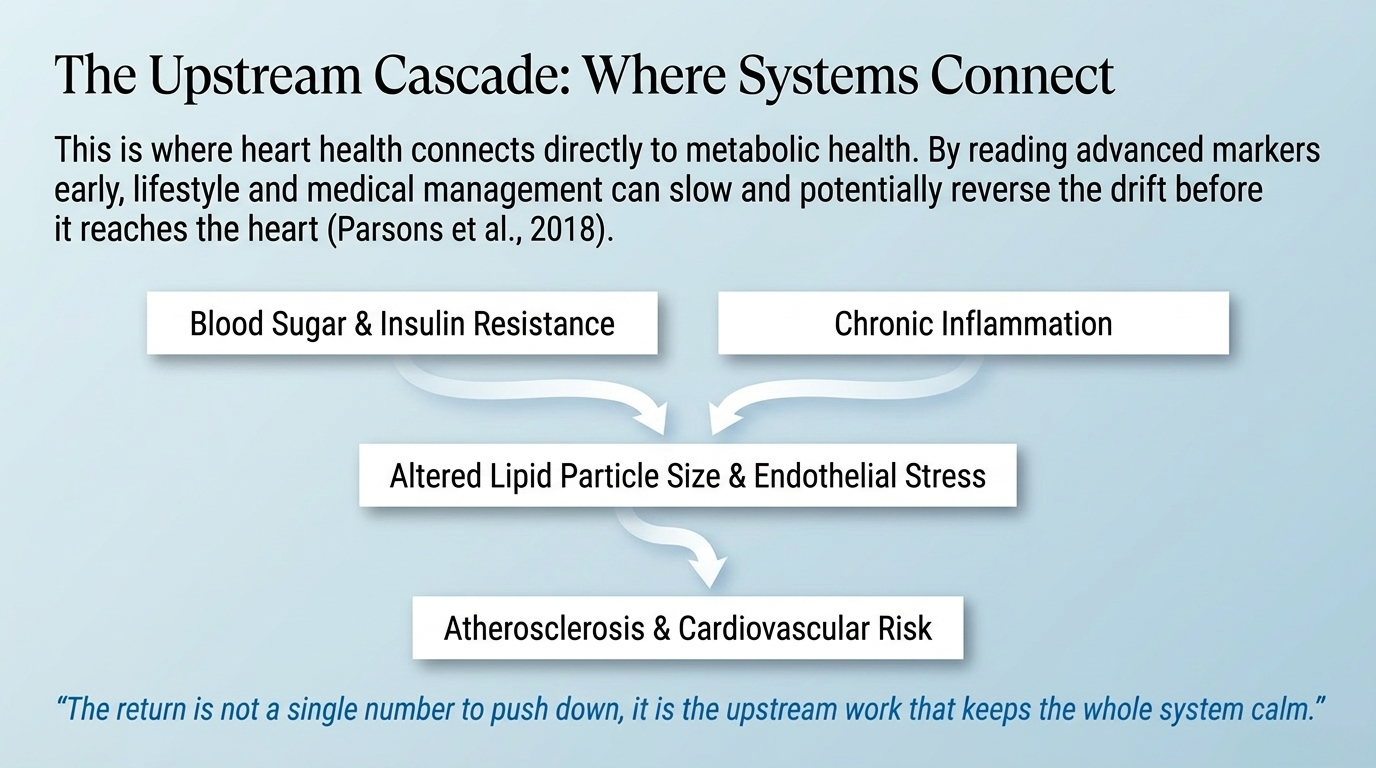
A healthy cardiovascular system holds a quiet baseline. Blood moves, vessels stay flexible, and the metabolic signals that govern them stay in range. Heart disease rarely begins at the heart. It begins upstream, in the slow drift of blood sugar, inflammation, and metabolic stress that shapes the vessels over years. Those early changes are signals worth reading long before a diagnosis. The return is not a single number to push down, it is the upstream work that keeps the whole system calm. What follows is how to think about the pieces, so you can have a better conversation with your own clinician.
How statins work, and how to weigh the tradeoffs
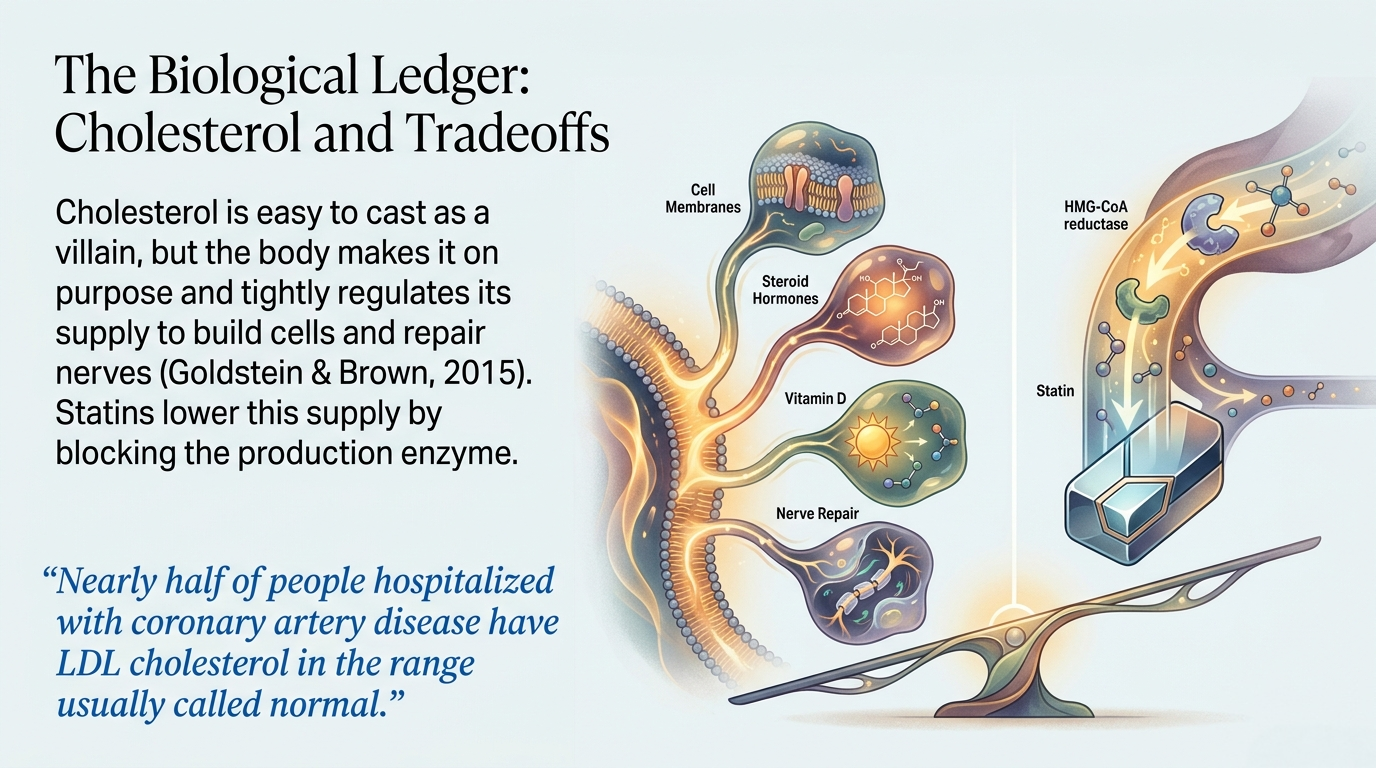
Statins lower cholesterol by blocking an enzyme the body uses to make it, a mechanism worked out over decades of cholesterol and cardiovascular science (Goldstein & Brown, 2015). The honest picture is one of tradeoffs, and part of that picture is that cholesterol numbers alone do not tell the whole story of risk. In a large analysis of people hospitalized with coronary artery disease, nearly half had LDL cholesterol in the range usually called normal (Sachdeva et al., 2009), and subclinical atherosclerosis is found even in people with normal LDL and no classic risk factors (Fernández-Friera et al., 2017). Some reviewers argue the LDL story is more complicated still (Ravnskov et al., 2018). The point of this section is not to tell you what to do, it is to help you understand the mechanism and the questions worth asking, so the decision you make with your clinician is an informed one.
Cholesterol, what it actually does
Cholesterol is easy to cast as the villain, but the body makes it on purpose. It builds cell membranes, it is the raw material for steroid hormones and vitamin D, and it supports nerve repair, which is why the body tightly regulates its own supply (Alphonse & Jones, 2016; Goldstein & Brown, 2015). That does not mean cholesterol never matters for heart risk, it means the story is more layered than a single high or low reading. Particle size and number, and the inflammation around them, shape risk more than the total number alone (Ference et al., 2020; Alizadeh-Fanalou et al., 2020; Libby et al., 2019). Understanding what cholesterol does makes the lab report easier to read with your clinician rather than to fear. Read the full guide →
Saturated fat and the diet-heart hypothesis
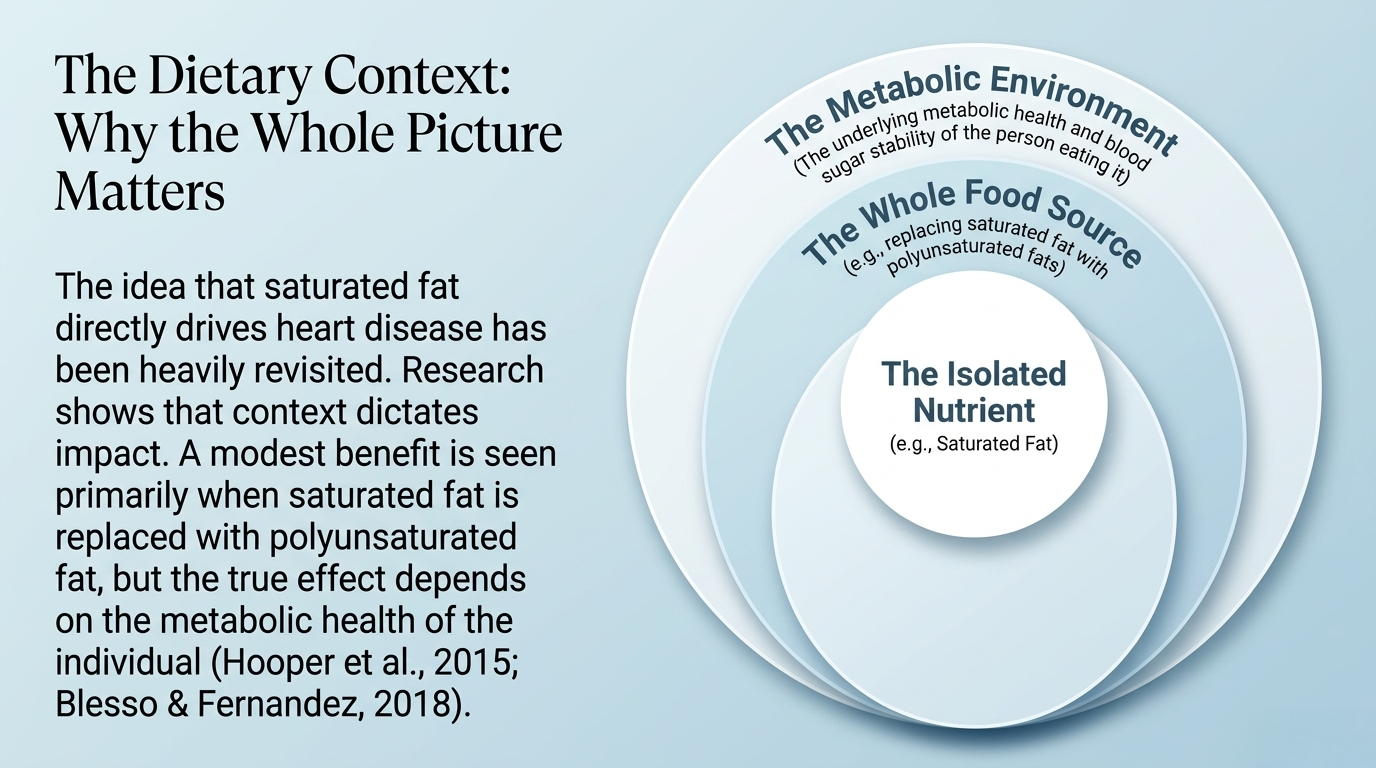
The idea that saturated fat directly drives heart disease, often called the diet-heart hypothesis, has been debated and revisited as the research has matured. A Cochrane review found that reducing saturated fat had a modest and uncertain effect on cardiovascular events, with benefit seen mainly when saturated fat was replaced with polyunsaturated fat (Hooper et al., 2015). Context matters, including the whole diet, the food source, and the metabolic health of the person eating it (Blesso & Fernandez, 2018; Vernooij et al., 2019). This is an area where reasonable experts still differ, so this section lays out the debate rather than declaring it settled, and points you toward a conversation with your clinician about your own diet.
Assessing cardiovascular risk functionally
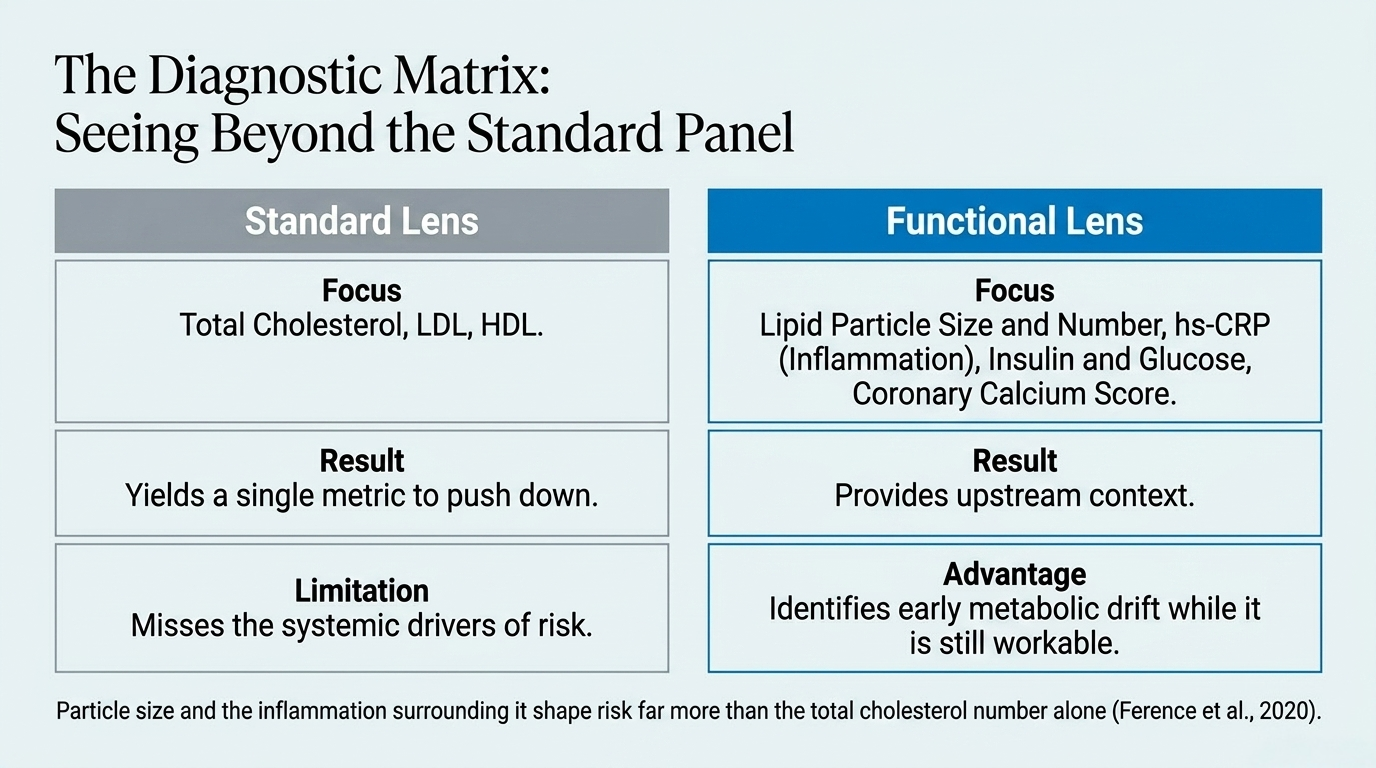
A standard cholesterol panel is a starting point, not the whole story. A functional assessment looks wider, at markers of inflammation, blood sugar and insulin, lipid particle counts, and imaging such as the coronary calcium score, read together rather than as a single number (Greenland et al., 2018; Jensen et al., 2014). The goal is to see the drift early, while it is still upstream and workable, and the encouraging news is that lifestyle and medical management can slow and in some cases reverse the process (Parsons et al., 2018). This is where heart health connects to your metabolic health.
Where these connect
Blood sugar
Insulin resistance and blood sugar drive cardiometabolic risk.
Inflammation
Chronic inflammation sits underneath atherosclerosis.
Testing
The advanced markers are a testing question, read against optimal ranges.
Frequently asked questions
How do statins actually work?
Statins block an enzyme the body uses to produce cholesterol, which lowers the amount circulating in the blood (Goldstein & Brown, 2015). Whether that lowering translates into meaningful benefit depends heavily on a person’s overall risk, which is why the conversation is individual. Talk with your clinician about your own situation.
Is high cholesterol always bad?
Not necessarily on its own. Cholesterol does essential work in the body, and risk is shaped by more than the total number, including particle size and number and the inflammation around it (Ference et al., 2020; Ravnskov et al., 2018). A fuller picture, read with a clinician, tells you more than one value.
Does saturated fat cause heart disease?
The link is more debated than the older simple message suggested. A Cochrane review found a modest, uncertain effect, mainly when replaced with polyunsaturated fat, and context matters (Hooper et al., 2015; Blesso & Fernandez, 2018). This is an area of ongoing discussion, so it is worth exploring with your own clinician rather than treating as settled.
What tests assess heart disease risk beyond cholesterol?
A functional assessment can include markers of inflammation, blood sugar and insulin, lipid particle counts, and the coronary calcium score, read against optimal ranges (Greenland et al., 2018; Jensen et al., 2014). These add context a standard panel alone can miss. See the testing guide for how to think about them.
References
Alizadeh-Fanalou, S., Nazarizadeh, A., Alian, F., et al. (2020). Small dense low-density lipoprotein-lowering agents. Biological Chemistry, 401(10), 1101-1121. https://doi.org/10.1515/hsz-2019-0426
Alphonse, P. A. S., & Jones, P. J. H. (2016). Revisiting human cholesterol synthesis and absorption. Lipids, 51(5), 519-536. https://doi.org/10.1007/s11745-015-4096-7
Blesso, C. N., & Fernandez, M. L. (2018). Dietary cholesterol, serum lipids, and heart disease: Are eggs working for or against you? Nutrients, 10(4), 426. https://doi.org/10.3390/nu10040426
Fernández-Friera, L., Fuster, V., López-Melgar, B., et al. (2017). Normal LDL-cholesterol levels are associated with subclinical atherosclerosis in the absence of risk factors. Journal of the American College of Cardiology, 70(24), 2979-2991. https://doi.org/10.1016/j.jacc.2017.10.024
Ference, B. A., Kastelein, J. J. P., & Catapano, A. L. (2020). Lipids and lipoproteins in 2020. JAMA, 324(6), 595. https://doi.org/10.1001/jama.2020.5685
Goldstein, J. L., & Brown, M. S. (2015). A century of cholesterol and coronaries: From plaques to genes to statins. Cell, 161(1), 161-172. https://doi.org/10.1016/j.cell.2015.01.036
Greenland, P., Blaha, M. J., Budoff, M. J., Erbel, R., & Watson, K. E. (2018). Coronary calcium score and cardiovascular risk. Journal of the American College of Cardiology, 72(4), 434-447. https://doi.org/10.1016/j.jacc.2018.05.027
Hooper, L., Martin, N., Abdelhamid, A., & Davey Smith, G. (2015). Reduction in saturated fat intake for cardiovascular disease. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD011737
Jensen, M. K., Bertoia, M. L., Cahill, L. E., et al. (2014). Novel metabolic biomarkers of cardiovascular disease. Nature Reviews Endocrinology, 10(11), 659-672. https://doi.org/10.1038/nrendo.2014.155
Libby, P., Buring, J. E., Badimon, L., et al. (2019). Atherosclerosis. Nature Reviews Disease Primers, 5(1), 56. https://doi.org/10.1038/s41572-019-0106-z
Parsons, C., Agasthi, P., Mookadam, F., & Arsanjani, R. (2018). Reversal of coronary atherosclerosis: Role of lifestyle and medical management. Trends in Cardiovascular Medicine, 28(8), 524-531. https://doi.org/10.1016/j.tcm.2018.05.002
Ravnskov, U., de Lorgeril, M., Diamond, D. M., et al. (2018). LDL-C does not cause cardiovascular disease: A comprehensive review of the current literature. Expert Review of Clinical Pharmacology, 11(10), 959-970. https://doi.org/10.1080/17512433.2018.1519391
Sachdeva, A., Cannon, C. P., Deedwania, P. C., et al. (2009). Lipid levels in patients hospitalized with coronary artery disease. American Heart Journal, 157(1), 111-117.e2. https://doi.org/10.1016/j.ahj.2008.08.010
Vernooij, R. W. M., Zeraatkar, D., Han, M. A., et al. (2019). Patterns of red and processed meat consumption and risk for cardiometabolic and cancer outcomes. Annals of Internal Medicine, 171(10), 732-741. https://doi.org/10.7326/M19-1583
Your life is your medicine.
Heart risk builds quietly and upstream, which is exactly why reading it early helps. If you want a place to begin, book a free 15 minute consult and we can talk through what your numbers and your history might mean, together.
